7914 - Neoplasm, malignant, any specified part of the endocrine system
DBQ: Link to Index of DBQ/Exams by Disability for DC 7914
Definition
A malignant neoplasm that gains access to tissue and spreads to other areas. It often recurs after attempts at surgical removal, and is also referred to as cancer.
{kind=link}
Etiology
The most common types are as follows:
-
Adrenals which are nonfunctional cancers, although rare, but can produce widespread processes behind and outside of the peritoneum. Tumors are metastatic in 30% of cases.
-
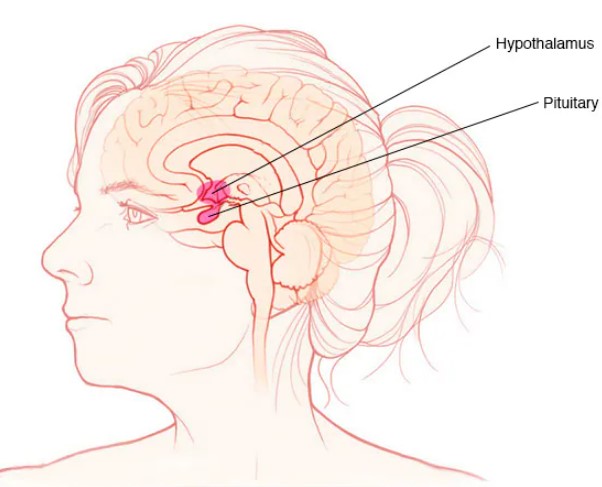
Hypothalamus which are most often affected by pituitary tumors. (See pituitary below).
-
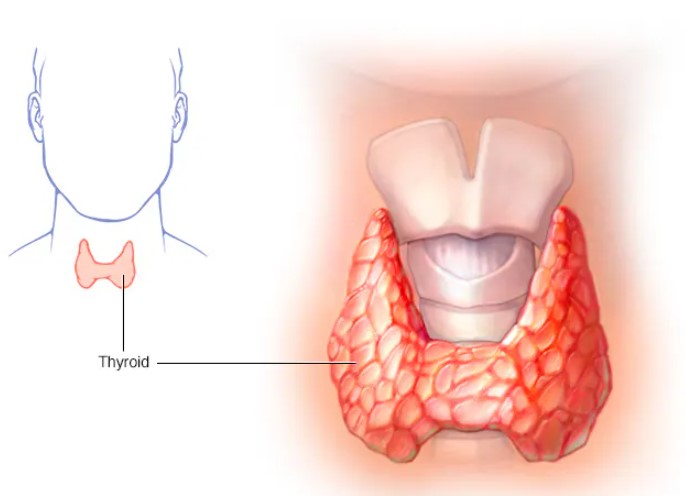
Thyroid which include four general types:
-
Papillary is the most common type. It occurs most often in patients with a history of radiation.
-
Follicular is more malignant than papillary carcinoma, but occurs less often. It is also occasionally associated with a history of radiation exposure.
-
Medullary involving secretion of excessive amounts of calcitonin which spread via the lymphatic and blood routes.
-
Anaplastic occurs mainly in individuals over 10 years of age. It accounts for less than 10% of thyroid cancers, and is characterized by rapid, painful enlargement of the thyroid. It may occur sporadically, or it may be seen in families.
-
-
Pituitary which include several theories regarding the etiology of the tumors. Rapid cell production or mutations in the cells are suggested as causes. In addition, inherited tendencies are also documented.
-
Pancreas which occur more frequently in men. Patients with a history of pancreatitis and a familial history of colon cancer syndromes without polyps are more susceptible.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Signs & Symptoms
Signs and symptoms of the common types of malignant tumors are as follows:
-
Adrenals - Adrenal insufficiency seldom occurs unless both glands are involved. Neoplasms less than 2 cm generate no symptoms. Signs of severe hemorrhage in both adrenals are abdominal pain, low hematocrit, and signs of acute adrenal failure. (See Diagnostic Code: 7911 Addison's Disease).
-
Hypothalmus -Tumors in this area cause: hypopituitarism, diabetes insipidus, and excessive secretion of prolactin (hyperprolactinemia).
-
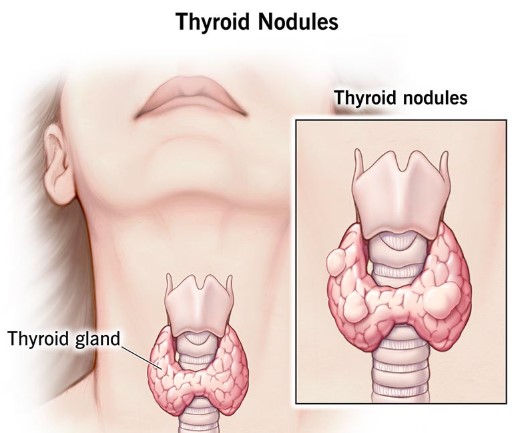
Thyroid - Malignant types of tumors occur most often in children or in patients over 60 years of age. The condition usually manifests as a single, hard, painless, rapid-growing nodule.
-
Pituitary - Many symptoms reflect effects of increased production of hormones. However, symptoms may occur secondary to the effects on surrounding tissues, e.g., headaches, visual field abnormalities, and decreased function of the gland related to compression of its structures. Decreased production of growth hormone, and hypogonadism occur.
-
Pancreatic - Symptoms in this type are related to the location of the tumor, and to whether or not it extends to other organs. Symptoms are usually vague, but include pain, jaundice, and weight loss, but rarely diabetes mellitus.
Tests
Tests related to the common types of tumors are as follows:
-
Adrenals - Computed tomography (CT) scan or magnetic resonance imaging (MRI) reveals the masses above the renal area. Upon the administration of an adrenocorticotropic hormone (ACTH) stimulation test, a failure of the plasma cortisol to increase and a failure of the urine to excrete cortisol demonstrate adrenal insufficiency.
-
Hypothalmus - Confirmation that compression from an extended tumor into the hypothalmus is the cause for hypopituitarism is received when the prolactin levels are low, and thyroid-stimulating hormone does not respond to thyrotropin-releasing hormone. In addition, the use of MRI or CT scanning with contrast medium is also used.
-
Thyroid - Evaluation of a thyroid nodule includes obtaining a history from the patient regarding previous exposure to radiation in the head and neck areas. Fine needle aspiration of the nodule to evaluate the tissue via cytology studies is the best diagnostic tool at this time. Thyroid function is evaluated by thyroid-stimulating hormone serum studies.
-
Pituitary - High resolution radiologic imaging, e.g., MRI is indicated to evaluate the tumor. Serum laboratory tests are done to evaluate pituitary function.
-
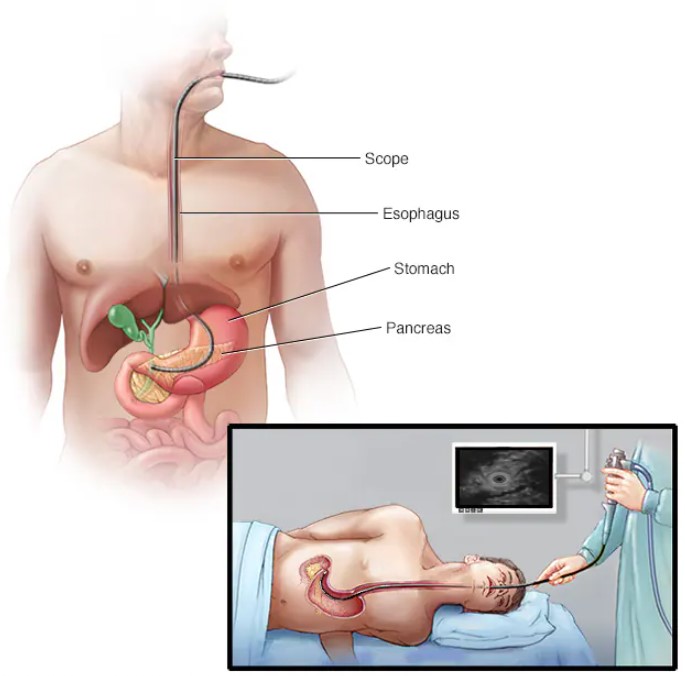
Pancreatic - No serological tests have been identified as routine to establish a diagnosis of pancreatic cancer. MRI is just starting to be used to make a diagnosis. Endoscopic ultrasounds and CT may be done.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Treatment
Treatments related to the common types of tumors are as follows:
-
Adrenals - Nonfunctional adrenal cancer usually spreads to other areas, and surgery is not helpful. However, chemotherapy, along with corticosteroid therapy, may provide some control.
-
Hypothalmus - Treatment for tumors stemming from the pituitary would include surgery to remove the tumor.
-
Thyroid - The surgical method varies from removing just the affected lobe to the near total removal of the thyroid. Ablation is used if parts of the tumor remain.
-
Pituitary - The primary method of treatment is surgery. Radiation may be used along with surgery, or medications, or by itself. Radiation is most commonly used if complete removal via surgery was not successful. Medical therapy is most often used in partnership with other therapies.
-
Pancreatic - Surgical removal of pancreatic cancerous tumors is the only means of obtaining a cure at this time. No single or combination of chemotherapeutic agents extends or improves the quality of life. Pain is controlled with analgesics or opiates or both. Malabsorption can be lessened with the use of medication with meals.
Residuals
-
Adrenals - Nonfunctional adrenal carcinoma is rare, but it produces a disseminated process occurring behind the peritoneum and outside the peritoneal cavity. Metastatic tumors account for 30% of nonfunctioning masses.
-
Hypothalmus - Hypopituitarism results in a decrease in the hormones it produces (see Diagnostic Code: 7907 Cushing's syndrome).
-
Thyroid - Following surgery, complications from permanent hypothyroidism develop. Vocal cord paralysis occurs in approximately 2% of the population.
-
Pituitary - In 50% of patients receiving surgery, hypopituitarism from large tumors is reversed in up to 50% of the patients. Cure rates depend on the size of the tumor. Tumors less than 1 cm have reportedly been corrected in 80 to 90% of patients. (See Diagnostic Code: 7907 Cushing's syndrome.)
-
Pancreatic - Only 10% of pancreatic cancers are operative, and of those that are operative, only 10% have a 5-year survival rate.
Special Considerations
-
Consider service connection on a presumptive basis as a chronic condition (38 CFR §3.307; §3.309 (a)).
-
Consider service connection on a presumptive basis as a condition associated with radiation exposure (38 CFR §3.307; §3.309 (d))
-
Consider service connection on a presumptive basis as a condition associated with ionizing radiation exposure (38 CFR §3.307; §3.309 (d); §3.311 (b)).
Notes
-
A rating of 100 percent shall continue beyond the cessation of any surgical, X-ray, antineoplastic chemotherapy or other therapeutic procedure. Six months after discontinuance of such treatment, the appropriate disability rating shall be determined by mandatory VA examination. Any change in evaluation based upon that or any subsequent examination shall be subject to the provisions of § 3.105(e) of this chapter. If there has been no local recurrence or metastasis, rate on residuals.